This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
PELVIC VARICOSE VEINS – VARICOCELE

DESCRIPTION
What is Pelvic Venous Insufficiency?
It is a broader concept which includes “pelvic varicose veins”. That is to say, the occurrence of varicose veins in the pelvis may come from primary insufficiency of the gonadal veins, or because there is an unusual compression of the retroperitoneal large venous vessels, such as the left renal vein (Nutcracker Syndrome), iliac veins (May-Thurner Syndrome), or because there is an insufficiency of the internal iliac vein branches, etc. Therefore, pelvic varicose veins are an indicator of something that may have different origins.
What are Pelvic Varicose Veins?
Just like the veins of the legs may suffer structural degeneration with development into varicose veins, either due to a familial-genetic issue or due to the sum of determining factors and lifestyle habits, pelvic veins may suffer exactly the same disorder and become and develop varicose plexus.
This is known as pelvic varicose veins or pelvic varicocele. Most commonly we observe these pelvic varicose veins, around the uterus and ovaries, in women who have had numerous pregnancies, or twin pregnancies, etc. Many female patients refer history of varicose veins in external genitals or in the internal side of the groin during pregnancy. Gonadal veins (ovarian in females, spermatic, in males) increase their calibre up to 10 times during gestation and although they use to return to a normal calibre, sometimes they do not do so and large venous axis remain (gonadal, ovarian) which become insufficient and develop, overtime, pelvic varicose veins.
The symptomatology they produce has the same pathophysiological explanation as in the varicose veins of the legs. In the pelvis, all this blood retention in the varicose veins and the inflammation that they develop may lead to chronic pain in the pelvis, in the pelvic floor, chronic congestion, feeling of diffuse inflammation, back and genital discomfort, pain during sexual intercourse (dyspareunia), similar symptoms to mild urinary infection (dysuria) and moreover leg heaviness almost always.
As it is not usual that the population is aware of this problem, which can lead to create poor quality of life, patients do not consult and do not think that it is about the same varicose vein problem but in a “superior stage”.
The existence of pelvic varicose veins in women is also known as pelvic varicocele or female varicocele, but may exist in men, although in this case these mentioned varicose veins usually do not lay in the pelvis itself (which may also occur) but in the testicles (typically in the left one) producing testicular varicocele, that may lead to sterility due to low quality sperm.
Moreover, varicose veins presence in the pelvis that depend on hypogastric venous territories, can easily be the cause of recurrent haemorrhoids, treatment which, besides the one performed by the general surgeon, should consist in sealing the internal starting point of these haemorrhoids, by pelvic venous embolisation.
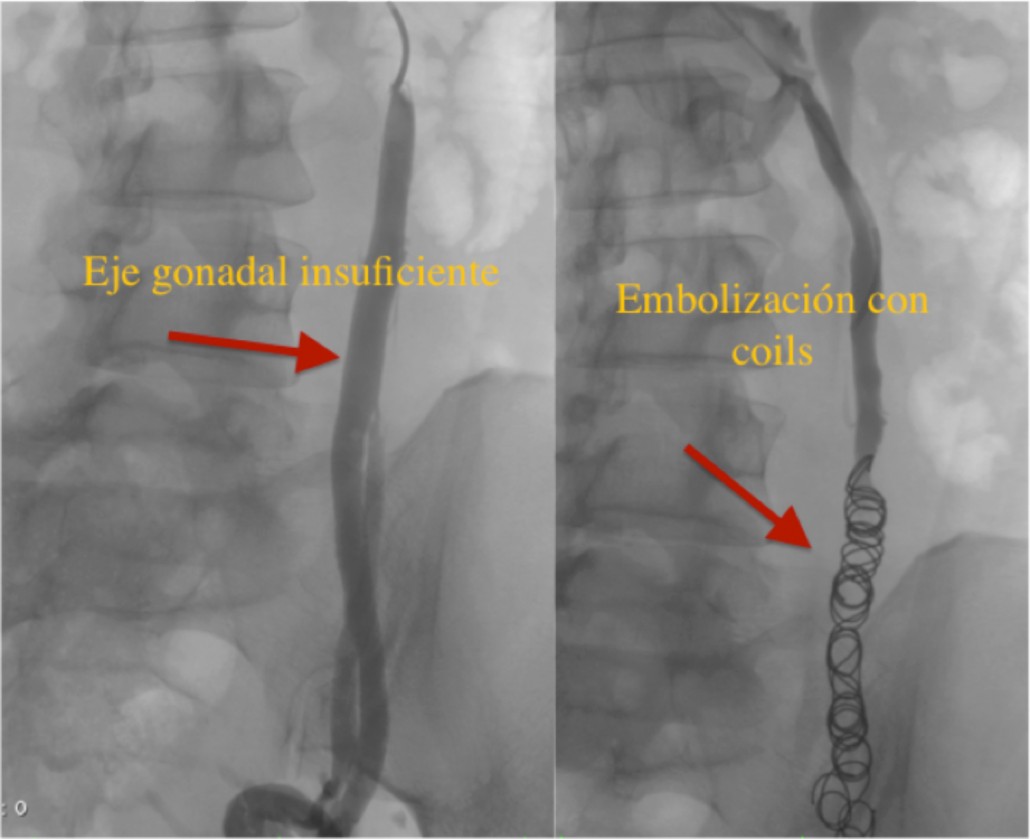
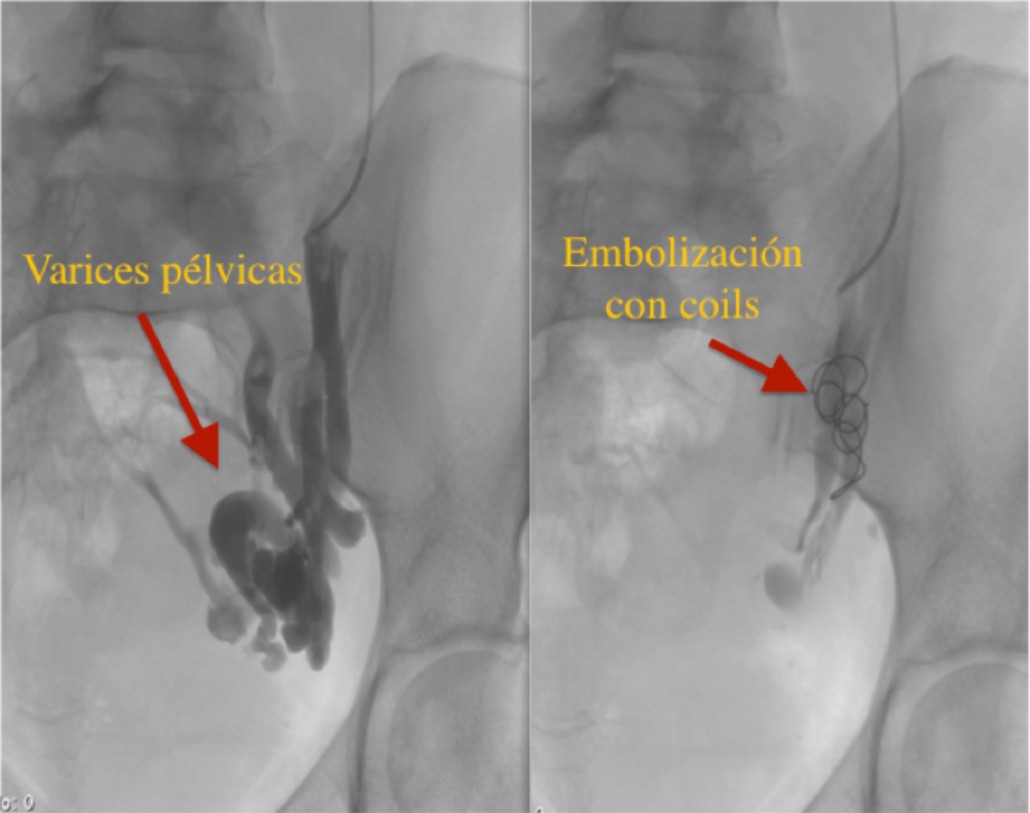
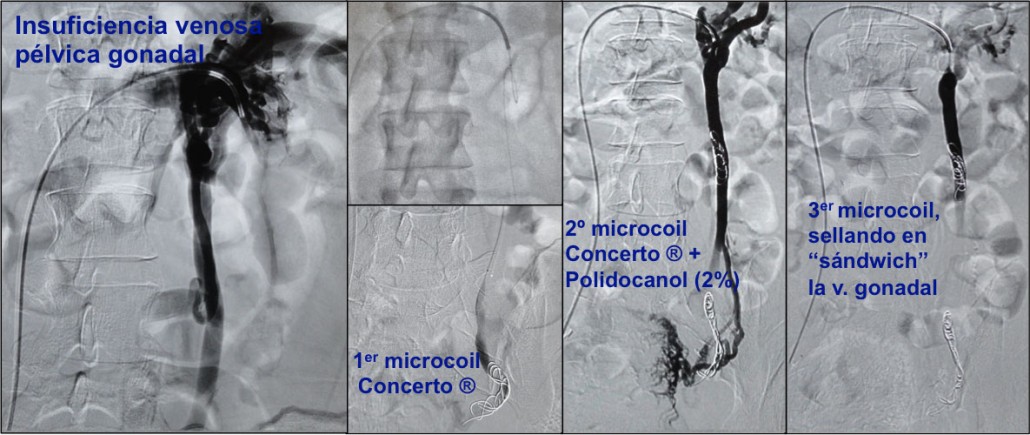
The treatment of these pelvic varicose veins and of varicocele is commonly performed by embolisation with spirals or coils, which are small filaments through which we block those varicose veins from the inside, by catheterization which is commonly performed from the arm and with local anaesthesia. It is a controlled procedure, safe and in more than 90% of the cases, very effective.
![]()